This web page was produced as an assignment for Genetics 677, an undergraduate course at UW-Madison.
Introduction
Juvenile Myelomonocytic Leukemia(JMML) is a form of leukemia that affects young children, typically under the age of 4. 25 to 50 of cases per year is the estimated number of cases. JMML is included in the category of Myelodysplastic and Myeloproliferative disorders by the World Health Organization [1]. There is no known environmental cause for the disease, however, 80% of patients have mutations in genes that code for leukemia cells which can be detected through laboratory testing.
The symptoms for JMML are nonspecific, and a child with JMML might exhibit any combination of pallor, fever, infection, bleeding, cough, poor weight gain, maculopapular rash, lymphadenophathy, moderate hepatomegaly, enlarged spleen, leukocytosis, monocytosis and thrombocytopenia. [2]
Stem cell (bone marrow) transplant is currently the only cure available for JMML patient, with about half the procedures being successes. However,, the risk of relapsing is also high at 50%, even if the initial operation was a success.[2][3] Transplants that are done at a younger age appear to have a higher success rate. Neither radiation therapy or chemotherapy alone is unable to bring about long term survival.
The symptoms for JMML are nonspecific, and a child with JMML might exhibit any combination of pallor, fever, infection, bleeding, cough, poor weight gain, maculopapular rash, lymphadenophathy, moderate hepatomegaly, enlarged spleen, leukocytosis, monocytosis and thrombocytopenia. [2]
Stem cell (bone marrow) transplant is currently the only cure available for JMML patient, with about half the procedures being successes. However,, the risk of relapsing is also high at 50%, even if the initial operation was a success.[2][3] Transplants that are done at a younger age appear to have a higher success rate. Neither radiation therapy or chemotherapy alone is unable to bring about long term survival.
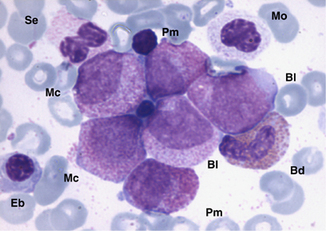
Bone marrow aspirate in Juvenile Myelomonocytic Leukemia (JMML)
KRAS and JMML

Location of Kras in Chromosome 12 in humans. [3]
The Kras gene is located on chromosome 12 and encodes a GTPase in humans. This GTPase, similar to many
other members of proteins coded by the Ras family, is an early player in
many signal transduction pathways.[4] Usually, the KRAS protein is
attached to the cell membrane. A mutated KRAS is very likely to be cancer
causing, possibly contributing to a variety of cancers including
JMML.[5]
JMML arises from the dysregulation of the Ras signaling pathway. This dysregulation causes the JMML cells to demonstrate hypersensitivity in vitro to granulocyte macrophage colony-stimulating factor (GM-CSF). Genes that are involved in the GM-CSF/Ras signaling pathway (including KRAS) accounts for up to 75% of JMML cases. The development of therapies and treatments for JMML is paved by the discovery of the involvement of the GM-CSF/Ras signaling pathway. [4]
JMML arises from the dysregulation of the Ras signaling pathway. This dysregulation causes the JMML cells to demonstrate hypersensitivity in vitro to granulocyte macrophage colony-stimulating factor (GM-CSF). Genes that are involved in the GM-CSF/Ras signaling pathway (including KRAS) accounts for up to 75% of JMML cases. The development of therapies and treatments for JMML is paved by the discovery of the involvement of the GM-CSF/Ras signaling pathway. [4]
Video
This is the first video of a series explaining some of the science behind JMML.
References
1) National Cancer Institute
http://www.cancer.gov/
2) JMML Foundation
http://www.jmmlfoundation.org/
3) Gene Cards
http://www.genecards.org/cgi-bin/carddisp.pl?gene=KRAS&search=KRAS
4) Juvenile myelomonocytic leukemia
http://www.ncbi.nlm.nih.gov/pubmed/15087069
5) McGrath JP, Capon DJ, Smith DH, Chen EY, Seeburg PH, Goeddel DV, Levinson AD (1983). "Structure and organization of the human Ki-ras proto-oncogene and a related processed pseudogene
6) Kranenburg O (November 2005). "The KRAS oncogene: past, present, and future". Biochim. Biophys.
7) Bone marrow aspirate in Juvenile Myelomonocytic Leukemia (JMML) - Pediatric Oncology Education Materials
http://pedsoncologyeducation.com/
http://www.cancer.gov/
2) JMML Foundation
http://www.jmmlfoundation.org/
3) Gene Cards
http://www.genecards.org/cgi-bin/carddisp.pl?gene=KRAS&search=KRAS
4) Juvenile myelomonocytic leukemia
http://www.ncbi.nlm.nih.gov/pubmed/15087069
5) McGrath JP, Capon DJ, Smith DH, Chen EY, Seeburg PH, Goeddel DV, Levinson AD (1983). "Structure and organization of the human Ki-ras proto-oncogene and a related processed pseudogene
6) Kranenburg O (November 2005). "The KRAS oncogene: past, present, and future". Biochim. Biophys.
7) Bone marrow aspirate in Juvenile Myelomonocytic Leukemia (JMML) - Pediatric Oncology Education Materials
http://pedsoncologyeducation.com/
The JMML foundation logo

